Where We Stand
Section: Sexual and Reproductive Health Care
Policy: Maternal Mortality and Morbidity as a Public Health Crisis
Appendix X
OMA Stance and National Implications
The OMA recognizes that maternal mortality and morbidity are of significant concern within Oregon and across the United States. The U.S. continues to fall behind peer countries in maternal health outcomes, with Black, American Indian and Alaskan Native (AIAN) and Native Hawaiian or Pacific Islander (NHPI) patients experiencing disproportionately high rates of maternal mortality.[i] Severe maternal morbidity rates are also higher among historically marginalized communities (with the highest being among Black women) compared to non-Hispanic white (NHW) women.[ii] Reproductive health policies and broader systemic factors, including income, housing stability, transportation, and racial disparities, further exacerbate these inequities. Significant shifts in federal policy due to changing government administrations have resulted in deleterious outcomes for patients. The recent overturning of abortion protections granted by Roe v. Wade in the 2022 Dobbs v. Jackson Women's Health Organization ruling transferred abortion regulatory power to individual states. Texas’s subsequent outlawing of abortion resulted in dramatically increased sepsis rates and mortality for pregnant patients.[iii],[iv] These complications disproportionally affect communities of color compounding with preexisting disparities.[v] This ruling illustrates the need to protect patient access to safe healthcare and for the OMA to establish policies that address maternal morbidity and mortality, with a focus on historically marginalized communities.
Defining Maternal Mortality and Morbidity
Maternal mortality is a public health crisis in the U.S. There are variations in the definition of maternal mortality, with the CDC and WHO defining it as death “while pregnant or within 42 days of ending of pregnancy, irrespective of the duration, and the site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management but not from accidental or incidental causes."[vi] The Oregon Health Authority however extends this timeline to include deaths within one year following pregnancy.[vii] The AMA supports the development of a standardized definition of maternal mortality and increased resource allocation to improve collection and analyze of maternal deaths.[viii] As per CDC data, in 2022, the US had 22 maternal deaths per 100,000 live births.[ix] Healthcare gaps that result in high maternal mortality rates disproportionately impact communities of color, particularly Black women, and have potentially deleterious downstream effects on newborn health and well-being.[x] The WHO defines maternal morbidity as “any health condition attributed to and/or complicating pregnancy, and childbirth that has a negative impact on the woman’s well-being and/or functioning”.[xi] Maternal morbidity is less researched than mortality, leading the true extent of maternal morbidity to be unknown.
Race Disparities within the United States
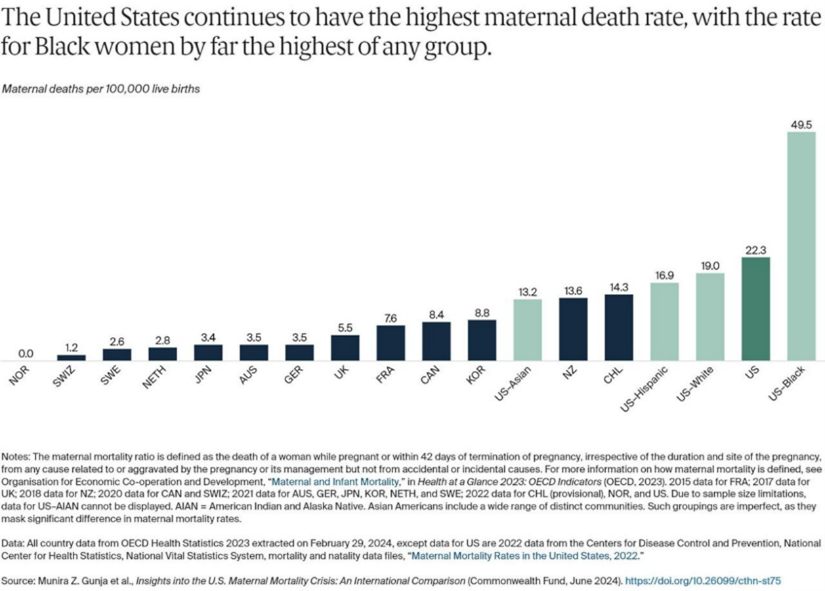
Maternal mortality rates fluctuate yearly, with a dramatic increase of 40% from 2020 to 2021 amid the COVID pandemic, but Black women have historically born the greatest burden.[xii] Using the WHO definition of maternal mortality, Black women experienced 69.9 maternal deaths/100,000 live births in 2021, and AIAN women had 63.4 maternal deaths/100,000 live births.[xiii] Although rates decreased the following year in 2022, Black women continued to be disproportionally affected, with 49.5 maternal deaths/100,000 live births, more than double the rate for white woman (19.0 maternal deaths/100,000 live births) [Figure 1].[xiv] This rate exceeds the combined maternal mortality rates of the next four highest-ranking countries: Chile at 14.3, New Zealand at 13.6, Korea at 8.8, and Canada at 8.4 [Figure 2].[xv]
Contributing Causes to Maternal Mortality
Over 80% of U.S. pregnancy-related deaths are preventable[xvi], illustrating the importance of recognizing both medical and systemic factors that contribute to maternal mortality. While Oregon performs better than the national rate, it was determined that between 2018-2020, 53% of pregnancy-related deaths were preventable in Oregon.[xvii] Black women and other women of color experience higher rates of pregnancy complications and mortality due in part to underdiagnosed chronic conditions, lack of a clinical protocol for identifying high-risk pregnancies, and inequitable treatment of these conditions.[xviii] For example, Black women frequently have higher risk for cardiovascular disease and are more likely to experience severe peripartum cardiomyopathy and end-organ damage due to hypertension with variable responses to hypertensive treatment compared to NHW women18. Additionally, when compared to NHW women, “Black, AIAN, and NHPI women have higher shares of preterm births, low birthweight births, or births for which they received late or no prenatal care.”[xix]
Maternal outcomes are also impacted by health determinants, which include individual behaviors, lifestyles, response to stress, genetics, epigenetics, clinical events, and social determinants such as economic stability, transportation access, and proximity to healthcare facilities.[xx] In the U.S., many regions lack access to an adequate number of maternity care providers, such as physicians, PAs, midwives, and doulas, leading to “maternity care deserts”.[xxi] This requires patients to travel long distances for basic obstetric care, something that many may not be able to do. The AMA supports promoting telehealth and home monitoring as a solution to provide remote patient care during and after pregnancy.[xxii] A lack of insurance and inadequate coverage from prenatal care through postpartum follow-up also contributes to high maternal mortality and morbidity rates in the United States .[xxiii] According to the 2021 U.S. Census Bureau, people of color are more likely to be uninsured than NHW individuals, making them particularly vulnerable to gaps in maternal care.[xxiv]
Structural racism and implicit bias within healthcare also contribute to poorer health outcomes for communities of color. Structural racism is described as the way systems - like housing, education, employment, media, criminal justice - reinforce discriminatory beliefs which then shape how resources are distributed.[xxv] Implicit biases are subconscious assumptions and behaviors about a group of people, often stemming from a lack of cultural understanding and education on the impact of disparities on health.25 The impact of structural racism and implicit bias is evident, as even when controlling for socioeconomic status and comorbidities, non-Hispanic Black women experience higher pregnancy-related complications compared to NHW women.25 Implicit bias can lead to microaggressions and discrimination, creating an environment that feels unsafe and furthering mistrust in medical systems, ultimately discouraging people from seeking care. Addressing these disparities to improve maternal outcomes requires improving patient-provider relationships through increased cultural humility training and disparity education for health care professionals.25
Strategies to Reduce Maternal Mortality Rates
A multifaceted approach is critical to improving patient care, with the goal of decreasing maternal mortality rates, and giving special attention to the unique disparities communities of color face. Key strategies should include:
- Improving Access to Quality Healthcare: Ensuring that high-quality prenatal and postpartum care is accessible for all patients that need it is crucial. This includes expanding Medicaid coverage to cover the entire 1-year postpartum period, which was enacted by the Oregon Health Authority in 2022.[xxvi] Medicaid expansion is linked to increased access to care, improved health outcomes, and reductions in racial disparities in healthcare.[xxvii]
- Addressing Racism and Implicit Bias: Training healthcare providers to recognize and address their own implicit biases, with the goal of lifelong work to equitable care, can improve quality of care that patients receive, especially those from historically marginalized groups[xxviii] and utilizing medical-legal partnerships to help health care providers and systems address the root causes of poor health outcomes[xxix].
- Medical Representation: Systemic factors, including racism, contribute to underrepresentation of certain races and ethnicities in the medical field. Patients of color are more likely to report lower quality patient-physician communication and participatory decision making when receiving care from racially discordant physicians.[xxx] Conversely, a study of hospital births in Florida found that newborn-physician race concordance was associated with a decrease in mortality of Black infants.[xxxi] Improving the recruitment and retention of clinicians from underrepresented communities not only improves the ability of healthcare to care for diverse patients but also improves patient outcomes.[xxxii]
- Enhancing Community Support: Strengthening community-based programs that provide support and health education can help improve outcomes. These programs can offer additional resources such as doulas, who contribute to the interprofessional maternity care team by providing continuous support during pregnancy, childbirth, and even postpartum care.[xxxiii] To improve postpartum care, Oregon is the first state that established Family Connects Oregon, a universally offered nurse home health visiting service for all families with newborns up to 6 months old.[xxxiv]
- Research and Data Collection: Increasing research on public health disparities, including Black, AIAN, and NHPI maternal mortality and morbidity rates, allows for comprehensive data collection to identify the specific needs and challenges faced by these women, thus informing more targeted interventions.[xxxv] The AMA also encourages state and county health departments to create maternal mortality surveillance systems.[xxxvi] Oregon established the Oregon Maternal Mortality and Morbidity Review Committee (MMRC) in 2018, which publishes a biennial report on maternal mortality and morbidity in Oregon.41
- Mental Health Services: In Oregon from 2018-2020, the most frequent cause for underlying cause of maternal death was mental health conditions, including substance use disorder (41%).[xxxvii] The shortage of mental health providers, insurance barriers, language differences, and geographical distances are some contributing factors of inadequate mental health services.37 Oregon’s MMRC recommends that actions are taken to ensure access to mental health services and substance use disorder services for pregnant and postpartum people, with a focus on the BIPOC community.37
- Policy Reformation: Implementing policies that screen for and address social determinant of health, by improving economic stability and access to education and housing, can help reduce disparities. This includes advocating for paid family leave and affordable childcare.[xxxviii]
- Public Awareness and Advocacy: Raising awareness about maternal mortality and its disparities with the goal of advocating for systemic changes can help drive policy reforms and increased support for impacted communities.35 It is crucial that this advocacy centers on engaging individuals with lived experiences of marginalization, whose personal expertise will guide change.[xxxix]
Conclusion
By addressing these areas of concern, we can work towards reducing the disparities in maternal health outcomes and ensuring that all women receive the care and support they need. These resolutions are supported in part by the American College of Obstetricians and Gynecologists and Oregon’s MMRC.37,39
Greater than 80% of pregnancy-related deaths were preventable.[xl] Access to adequate healthcare improves health outcomes for pregnant mothers. Structural racism and implicit bias contribute to the disparate maternal mortality outcomes for Black, AIAN and NHPI mothers. Strategies to implement culturally humility have been shown to improve health outcomes for pregnant women. Health determinants have a significant negative impact on maternal health outcomes. Strategies that directly address health determinants, such as medical-legal partnerships[xli]52, can support pregnant and postpartum mothers by providing legal assistance to address issues that may impact their health including housing, eviction, food insecurity, medication access and health insurance coverage, or other financial challenges.
Figure 1: “Maternal mortality rate, by race and Hispanic origin: United States, 2021 and 2022”
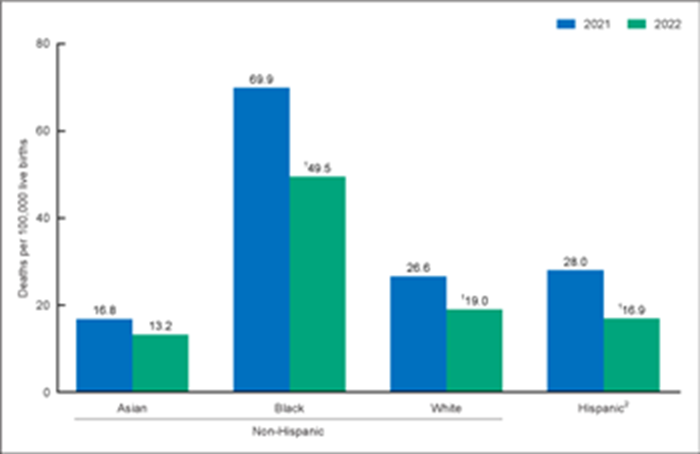
Figure 2
[i] 1.Gunja M, Gumas E, Masitha R, Zephyrin L. Insights into the U.S. Maternal Mortality Crisis: An International Comparison. The Commonwealth Fund. Published June 4, 2024. https://www.commonwealthfund.org/publications/issue-briefs/2024/jun/insights-us-maternal-mortality-crisis-international-comparison
[ii] Howell EA. Reducing Disparities in Severe Maternal Morbidity and Mortality. Clin Obstet Gynecol. 2018;61(2):387-399. doi:10.1097/GRF.0000000000000349
[iii] Suozzo,Sophie, A. (2025, February 20). Texas Won’t Study How Its Abortion Ban Impacts Women, So We Did. Retrieved March 25, 2025, from ProPublica website: https://www.propublica.org/article/texas-maternal-mortality-analysis-methodology
[iv] Presser,Andrea, L. (2025, February 20). Texas Banned Abortion. Then Sepsis Rates Soared. Retrieved March 25, 2025, from ProPublica website: https://www.propublica.org/article/texas-abortion-ban-sepsis-maternal-mortality-analysis
[v] Abrams, Z. (2023, April 14). Abortion Bans Cause Outsized Harm for People of Color. Retrieved March 25, 2025, from American Psychological Association website: https://www.apa.org/monitor/2023/06/abortion-bans-harm-people-of-color
[vi] Cresswell, J. (2025). Maternal deaths. Retrieved March 25, 2025, from World Health Organization website: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/4622
[vii] Oregon Health Authority. (2023). January 2023 biennial report: Maternal mortality review committee (MMRC). Retrieved from https://www.oregon.gov/oha/PH/HEALTHYPEOPLEFAMILIES/DATAREPORTS/MCHTITLEV/Documents/January2023BiennielReportMMRCFinal.pdf . Accessed March 25, 2025.
[viii] American Medical Association. (n.d.). Reducing inequities and improving access to insurance for maternal health care (H-185.917). Retrieved from https://policysearch.ama-assn.org/policyfinder/detail/%22Reducing%20Inequities%20and%20Improving%20Access%20to%20Insurance%20for%20Maternal%20Health%20Care%20%20H-185.917%22?uri=%2FAMADoc%2FHOD.xml-H-185.917.xml. Accessed March 25, 2025.
[ix] Centers for Disease Control and Prevention. (2022). Maternal mortality rates, 2022. Retrieved from https://www.cdc.gov/nchs/data/hestat/maternal-mortality/2022/maternal-mortality-rates-2022.htm. Accessed March 25, 2025.
[x] Howell, E. A. (2018). Reducing disparities in severe maternal morbidity and mortality. Clinical Obstetrics and Gynecology, 61(2), 387–399. doi:10.1097/GRF.0000000000000349. Accessed March 25, 2025.
[xi] World Health Organization. (n.d.). Maternal morbidity and well-being. Retrieved from https://www.who.int/teams/maternal-newborn-child-adolescent-health-and-ageing/maternal-health/maternal-morbidity-and-well-being. Accessed March 25, 2025.
[xii] Katella, K. (2023, May 22). Maternal Mortality Is on the Rise: 8 Things to Know. Retrieved March 25, 2025, from Yale Medicine website: https://www.yalemedicine.org/news/maternal-mortality-on-the-rise
[xiii]Centers for Disease Control and Prevention. (2021). Maternal mortality rates, 2021. Retrieved from https://www.cdc.gov/nchs/data/hestat/maternal-mortality/2021/maternal-mortality-rates-2021.htm. Accessed March 25, 2025.
[xiv]Britt, R. (2025, February 7). Maternal Mortality in the U.S Declined, though Disparities in the Black Population Persist - Policy Center for Maternal Mental Health. Retrieved March 25, 2025, from Policy Center for Maternal Mental Health website: https://policycentermmh.org/maternal-mortality-in-the-u-s-a-declining-trend-with-persistent-racial-disparities-in-the-black-population/
[xv] Gunja, M., Gumas, E., Masitha, R., & Zephyrin, L. (2024, June 4). Insights into the U.S. Maternal Mortality Crisis: An International Comparison. Retrieved March 25, 2025, from The Commonwealth Fund website: https://www.commonwealthfund.org/publications/issue-briefs/2024/jun/insights-us-maternal-mortality-crisis-international-comparison
[xvi]CDC. (2024, May 30). Pregnancy-Related Deaths: Data From Maternal Mortality Review Committees in 36 U.S. States, 2017–2019. Retrieved March 25, 2025, from Maternal Mortality Prevention website: https://www.cdc.gov/maternal-mortality/php/data-research/mmrc-2017-2019.html?CDC_AAref_Val=https://www.cdc.gov/reproductivehealth/maternal-mortality/erase-mm/data-mmrc.html
[xvii]Oregon Maternal Mortality and Morbity Review Committee Biennial Report. (2023). Retrieved from https://www.oregon.gov/oha/PH/HEALTHYPEOPLEFAMILIES/DATAREPORTS/MCHTITLEV/Documents/January2023BiennielReportMMRCFinal.pdf
[xviii]Montalmant, K.E., Ettinger, A.K. The Racial Disparities in Maternal Mortality and Impact of Structural Racism and Implicit Racial Bias on Pregnant Black Women: A Review of the Literature. J. Racial and Ethnic Health Disparities 11, 3658–3677 (2024). https://doi-org.proxy.westernu.edu/10.1007/s40615-023-01816-x
[xix] Hill, L., Artiga, S., Ranji, U., & Rao, A. (2024, October 25). Racial Disparities in Maternal and Infant Health: Current Status and Efforts to Address Them. Retrieved March 25, 2025, from Kaiser Family Foundation website: https://www.kff.org/racial-equity-and-health-policy/issue-brief/racial-disparities-in-maternal-and-infant-health-current-status-and-efforts-to-address-them/
[xx] Racial and Ethnic Inequities in Obstetrics and Gynecology. (2024). Retrieved March 25, 2025, from Acog.org website: https://www.acog.org/clinical/clinical-guidance/committee-statement/articles/2024/09/racial-and-ethnic-inequities-in-obstetrics-and-gynecology
[xxi]Sonenberg, A., & Mason, D. J. (2023). Maternity Care Deserts in the US. JAMA Health Forum, 4(1), e225541. https://doi.org/10.1001/jamahealthforum.2022.5541
[xxii] AMA recommendations to improve maternal health outcomes. (2024, August 30). Retrieved March 26, 2025, from American Medical Association website: https://www.ama-assn.org/delivering-care/public-health/ama-recommendations-improve-maternal-health-outcomes#
[xxiii] Zundel, R. (2022). Inadequate Maternal Health Care for Women in the United States. Retrieved March 26, 2025, from Ballard Brief website: https://ballardbrief.byu.edu/issue-briefs/inadequate-maternal-health-care-for-women-in-the-united-states
[xxiv]Branch, B., & Conway, D. (2022). Health Insurance Coverage by Race and Hispanic Origin: 2021. Retrieved from https://www.census.gov/content/dam/Census/library/publications/2022/acs/acsbr-012.pdf
[xxv]Montalmant, K.E., Ettinger, A.K. The Racial Disparities in Maternal Mortality and Impact of Structural Racism and Implicit Racial Bias on Pregnant Black Women: A Review of the Literature. J. Racial and Ethnic Health Disparities 11, 3658–3677 (2024). https://doi-org.proxy.westernu.edu/10.1007/s40615-023-01816-x
[xxvi] Inbody, D. (2022). 12-month eligibility for Oregon Health Plan post-partum benefits. Retrieved from https://www.oregon.gov/oha/HSD/OHP/Announcements/12-month%20eligibility%20for%20Oregon%20Health%20Plan%20post-partum%20benefits.pdf
[xxvii]Racial and Ethnic Inequities in Obstetrics and Gynecology. (2024). Retrieved March 25, 2025, from Acog.org website: https://www.acog.org/clinical/clinical-guidance/committee-statement/articles/2024/09/racial-and-ethnic-inequities-in-obstetrics-and-gynecology
[xxviii]Crear-Perry J, Correa-de-Araujo R, Lewis Johnson T, McLemore MR, Neilson E, Wallace M. Social and Structural Determinants of Health Inequities in Maternal Health. J Womens Health (Larchmt). 2021;30(2):230-235. doi:10.1089/jwh.2020.8882
[xxix]Home -- National Center for Medical-Legal Partnership. (n.d.). Retrieved March 26, 2025, from Medical-Legal Partnership website: https://medical-legalpartnership.org/
[xxx]Shen MJ, Peterson EB, Costas-Muñiz R, Hernandez MH, Jewell ST, Matsoukas K, et al. The effects of race and racial concordance on patient-physician communication: a systematic review of the literature. J Racial Ethn Health Disparities 2018; 5: 117– 40. doi: 10.1007/s40615-017-0350-4
[xxxi] Greenwood BN, Hardeman RR, Huang L, Sojourner A. Physician-patient racial concordance and disparities in birthing mortality for newborns. Proc Natl Acad Sci U S A 2020; 117: 21194– 200. doi: 10.1073/pnas.1913405117
[xxxii]St. George's University. (2018, December 17). The Importance of Diversity in Health Care. Retrieved March 26, 2025, from Sgu.edu website: https://www.sgu.edu/blog/medical/pros-discuss-the-importance-of-diversity-in-health-care/
[xxxiii]Improving Maternal and Infant Health Through Multisector, Community-Driven Partnerships. (2024). Commonwealthfund.org. https://doi.org/10.26099/rfyp-4k12
[xxxiv]Oregon Health Authority : Family Connects Oregon : Home Visiting : State of Oregon. (n.d.). Retrieved March 26, 2025, from Oregon.gov website: https://www.oregon.gov/oha/PH/HEALTHYPEOPLEFAMILIES/BABIES/HOMEVISITING/Pages/Family-Connects-Oregon.aspx
[xxxv]Purandare, R. (2023, August 10). Addressing Maternal Mortality Through Improved Data Collection and Access | AcademyHealth. Retrieved March 26, 2025, from academyhealth.org website: https://academyhealth.org/blog/2023-08/addressing-maternal-mortality-through-improved-data-collection-and-access
[xxxvi]Policy Finder | AMA. (2025). Retrieved March 26, 2025, from Ama-assn.org website: https://policysearch.ama-assn.org/policyfinder/detail/Maternal%20Morbidity?uri=%2FAMADoc%2Fdirectives.xml-0-1423.xml
[xxxvii]Oregon Maternal Mortality and Morbity Review Committee Biennial Report. (2023). Retrieved from https://www.oregon.gov/oha/PH/HEALTHYPEOPLEFAMILIES/DATAREPORTS/MCHTITLEV/Documents/January2023BiennielReportMMRCFinal.pdf
[xxxviii]Crear-Perry J, Correa-de-Araujo R, Lewis Johnson T, McLemore MR, Neilson E, Wallace M. Social and Structural Determinants of Health Inequities in Maternal Health. J Womens Health (Larchmt). 2021;30(2):230-235. doi:10.1089/jwh.2020.8882
[xxxix]Racial and Ethnic Inequities in Obstetrics and Gynecology. (2024). Retrieved March 25, 2025, from Acog.org website: https://www.acog.org/clinical/clinical-guidance/committee-statement/articles/2024/09/racial-and-ethnic-inequities-in-obstetrics-and-gynecology
[xl] CDC. (2024, September 25). Preventing Pregnancy-Related Deaths. Retrieved March 26, 2025, from Maternal Mortality Prevention website: https://www.cdc.gov/maternal-mortality/preventing-pregnancy-related-deaths/index.html
[xli] AMA recommendations to improve maternal health outcomes. (2024, August 30). Retrieved March 26, 2025, from American Medical Association website: https://www.ama-assn.org/delivering-care/public-health/ama-recommendations-improve-maternal-health-outcomes#